RA Medication: Advanced DMARDs
Over the last two decades, we have had a number of sophisticated medications genetically engineered to work on specific targets in the immune system. These are called biologic DMARDs (bDMARDs).
Even more recently, powerful oral medications have been developed to work within the immune cells, to disrupt the cell-signalling processes which lead to the inflammatory and immune responses seen in RA. These are called targeted synthetic DMARDs.
The Modern Era Of Treatments for Inflammatory Arthritis
With the new group of biologic and targeted synthetic DMARDs available, few rheumatologists will linger on the older generation drugs once it is clear remission or at least, a very low level of disease activity, cannot be attained using these conventional DMARDs and/or anti-inflammatory medications.
Since 2004, people in Australia with inflammatory arthritis have had good access to biologic DMARD medications, with the costs heavily subsidised by our government.
This has clearly helped rheumatologists achieve better outcomes for people with the disease who have not been doing well enough on the conventional DMARDs.
The problem is the high monetary costs of these agents. While it’s unsavoury for some to have to compromise on treatment due to cost, this is an increasing reality given the limited health dollar in all nations.
Strategies to use these high cost, highly effective medications in the most efficient and cost-effective manner are being investigated.
In addition, there is immense interest in developing ways to be more precise in how we use medications in any given individual so that we can really have good results without side effects. The goal should be to use the right drug in the right person at the right time.
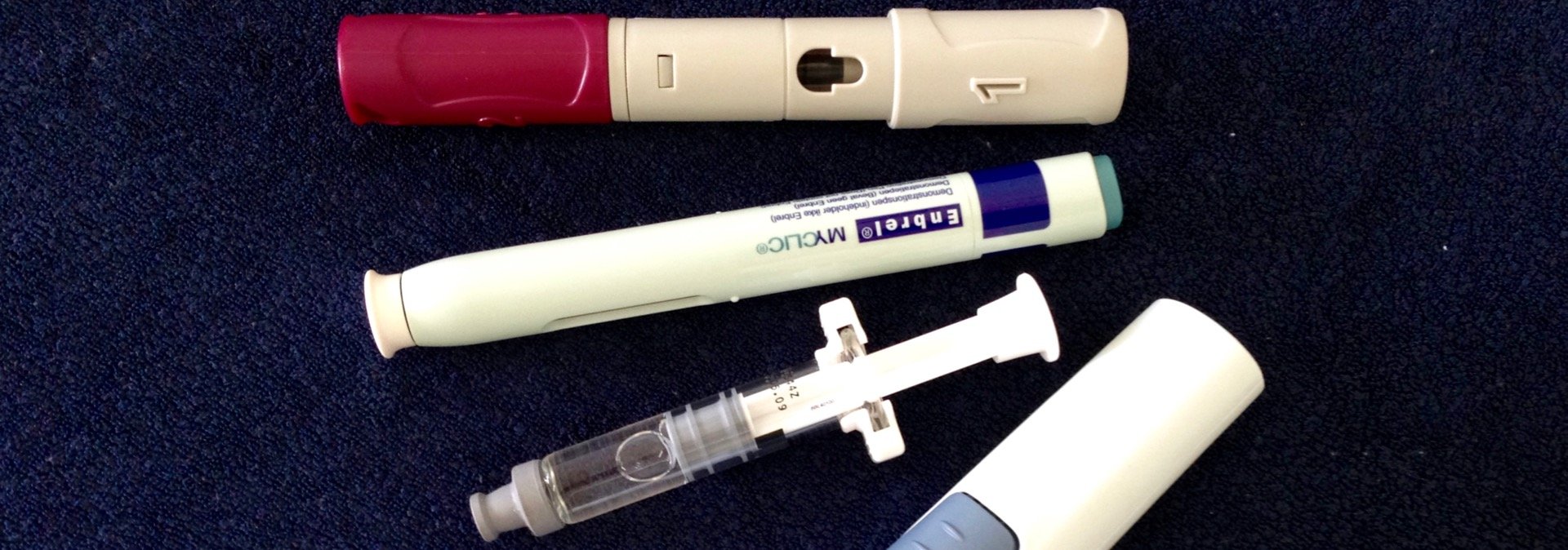
Biologic DMARDs
The class of these drugs which have been around the longest is the tumour necrosis factor (TNF) inhibitors. Medications in this class include Etanercept, Adalimumab, Infliximab, Certolizumab pegol, and Golimumab.
TNF inhibitors have been shown to be effective across many different diseases, including RA, PsA and AS.
For RA, there are a variety of other medications which work differently by interfering with different targets to dampen the overactive autoimmune response. These include Abatacept (CTLA4-Ig), Rituximab (anti-CD20 antibody), and Tocilizumab (anti-IL6 receptor antibody).
For PsA and AS, we also have the IL-17 inhibitors, Secukinumab and Ixekizumab.
For psoriatic arthritis, there is also the IL12/23 inhibitor, Ustekinumab.
Biologic DMARDs Blogs