

Carpal tunnel syndrome is common. After feeling pain, tingling, numbness and/or weakness in the hand for some time, the sufferer seeks some medical advice.
The diagnosis can be made by the description of symptoms and a physical examination of the wrist and hand.
It's common for patients to have a nerve conduction study, which is a test that helps work out if the median nerve is irritated or damaged. This nerve sits in the carpal tunnel (click for anatomy) with pressure on the nerve leading to the symptoms.
Treatment tends to be directed at avoiding aggravating activity, the use of wrist splints, and then, surgery to the carpal tunnel to take pressure off the median nerve if conservative measures do not work.
As a rheumatologist, I see a skewed number of patients with carpal tunnel syndrome who may not need or may not have needed carpal tunnel surgery.
I write a lot about inflammatory arthritis. When people, including doctors, think about an arthritis, they concentrate on joint disease. But, it's equally important to think of the tendons. The tendons may swell. Their coverings or lining, the sheaths, can become very inflamed.
Now, the carpal tunnel contains the median nerve and a whole bunch of tendons, tendons which work to flex your fingers.
When the tendons and their sheaths are affected by the underlying inflammatory arthritis, they swell and the space within the carpal tunnel gets tighter and tighter, with the median nerve becoming squashed.
This happens with rheumatoid arthritis. It happens with psoriatic arthritis and spondyloarthritis. It can happen with many of the inflammatory diseases rheumatologist treat.
In these cases, surgery may well not be required.
We would aim to reduce the swelling within the tunnel. A cortisone injection directed to the inflamed, swollen area can help settle the problem as an adjunct to longer term treatment of any underlying disease.
Underlying inflammatory arthritis presenting as carpal tunnel syndrome is often not picked up early.
A simple, readily available examination which would quickly show the state of the nerve and the underlying tendons is an ultrasound. It does however require the health professional assessing the problem to be cognizant that inflammatory causes exist.
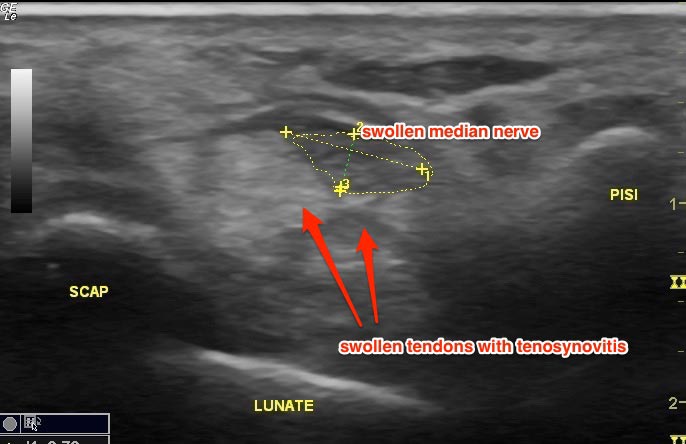 Ultrasound Image: Cross-section of Carpal Tunnel. (SCAP = scaphoid, PISI = pisiform)
Ultrasound Image: Cross-section of Carpal Tunnel. (SCAP = scaphoid, PISI = pisiform)
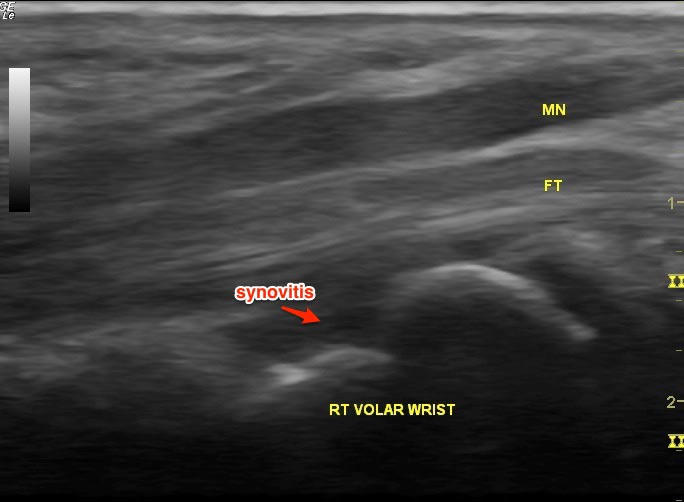 Ultrasound Image: Longitudinal view (MN = median nerve, FT = flexor tendon)
Ultrasound Image: Longitudinal view (MN = median nerve, FT = flexor tendon)
I think there are some situations where more investigation or considered thought should occur prior to surgery. These include:
- a person presenting with BOTH hands being affected. Suspicious.
- when the carpal tunnel symptoms occur in the setting of other joint problems (especially if there is already a known rheumatological diagnosis). This requires a careful history.
- when it occurs in a young individual for no apparent reason. By that I mean, there's no obvious aggravating activity to cause the problem.
What's your experience with carpal tunnel syndrome?
