In rheumatology, there are few super-urgent, “life or death” situations. I like it that way.
Most times when urgency is involved, it’s usually relates to a severe side effect or to a severe infection. Rarely, it relates to the manifestations of difficult disease processes, such as vasculitis (where there is inflammation of blood vessels causing a lack of blood supply to the organs the vessel supplies).
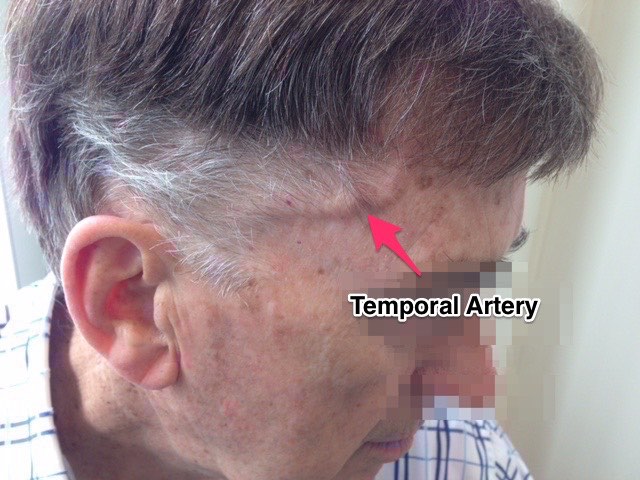
Last week, I took an urgent call from a local GP. She’s a very astute GP and when faced with this older gentleman presenting with headaches, fever, a feeling of being unwell as well as a lot of tenderness at his right scalp, she immediately suspected this relatively rare disease.
Giant Cell Arteritis (read more about GCA here).
This is an emergency situation and should be treated as such.
Giant Cell Arteritis can lead to sudden, permanent loss of vision and prompt treatment can prevent it.
We discussed his case over the phone and these were organised urgently:
What about my role as a rheumatologist?
Well, the good news with this disease is that the use of corticosteroid, Prednisone, helps immensely. The problem is that the antidote is Prednisone. I’ve already written about the 2-edged sword that Prednisone can be (here's a link to posts re corticosteroid). And this is definitely the case at these higher doses.
So, in this disease, the rheumatology management consists of:
All this needs to be done, while trying not to reduce Prednisone too quickly to avoid a flare in the disease, as a lack of control on the inflammation causes many unwanted symptoms, and in particular, increases that risk of sudden blindness.
Have you any experience of this condition?
{kind=link}